
This post is about one of an important condition, we come across in gynaecology oncology and that is Lynch Syndrome. Recently there has been evidence found for it to be strongly associated with endometrial and ovarian cancer. NICE recommends to screen all women with endometrial cancer for Lynch syndrome. The points are taken from a recently published TOG which is free access.
To download the original article: Click Here
For infographic: Click Here
 |
Introduction
- Lynch syndrome (LS) → an autosomal dominant inherited condition
- Predisposes to cancers which include colorectal, endometrial & ovarian
- Most affected 95% people are unaware of their risk
- Gynecological cancer → often the first cancer diagnosis in women
Epidemiology
- Exact prevalence → unclear 1:278 to 1:440
- LS is the most common inherited cancer predisposition syndrome
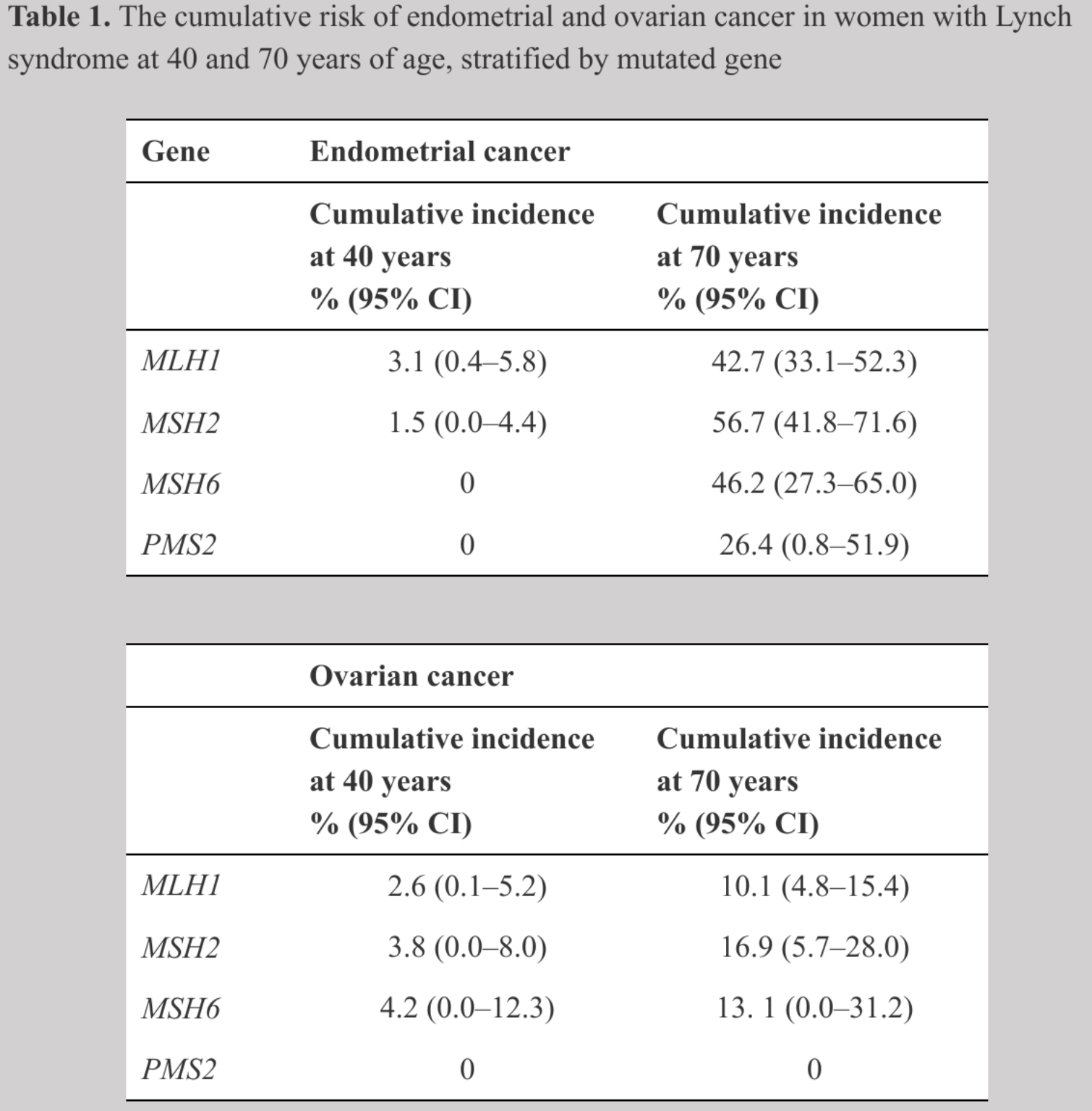
- Around 3% endometrial cancers are due to LS prognosis very good 10-yr survival ≥90%
- Association with ovarian cancer less clear 1-2%
- NICE recommends universal screening of individuals with colorectal cancer and endometrial cancer
- Degree of penetrance, disease spectrum and age of cancer onset variable
Lynch Syndrome
- Arises from inherited mutations in genes encoding proteins of highly conserved DNA mismatch repair (MMR) system MLH1, MSH2, MSH6 & PMS2
- MMR system maintains genomic stability
- Without functioning MMR→ uncorrected mutation rate ↑ by 1000-fold
How does it happen?
- One pathogenic allele of an MMR gene is inherited & once second allele acquires somatic inactivating mutation→ as MMR system is non-functional which leads to widespread genomic instability as errors which occur during replication can not be corrected
- Hypermutation leads to carcinogenesis
- Incidence of endometrial cancer in (MSH6 = MLH1 & MLH2) > PMS2
 |
| Ref:TOG |
Colorectal cancer and LS
- The most common & lethal cancer in LS carriers→ colorectal
- Risk depends on affected gene & gender less in ♀
- Lifetime risk MLH1 variant 47% PMS2 variant 14%
- Earlier onset with median age 52 yrs (69 yrs in sporadic)
- more on the right side of colon
Bedrock of management Biennial colonscopic colorectal surveillance
- With high quality surveillance→ significant reduction in deaths
- Often extensive surgery required
For gynaecologist
- Main point in counselling→ need for regular colonoscopies
- Coordinate surveillance & surgery with colorectal colleagues
- MDT approach
Ref: TOG
Risk-reducing strategies for LS
- ♀with LS should be seen by 25 yrs by an expert gynaecologist
Women with completed family → TAH + BSO as lifetime risk of gynae cancer is sufficiently high
- Timing of surgery→ gene-specific
- Survival benefits achieved by risk-reducing surgery→ minimal (as LS associated endometrial & ovarian cancer have good prognosis I)
- However, many prefer to have risk-reducing surgery
- Preferred approach→ laparoscopic
- Hysterectomy should be coordinated with other risk-reducing interventions e.g. colonoscopy or colorectal surgery
- TAH + BSO at 40 yrs is cost effective
HRT in the form of transdermal patches as estrogen is protective for colorectal & endometrial carcinoma & does not appreciably ↑risk of breast cancer
OCPs ↓ risk of sporadic endometrial & ovarian cancers as well as BRCA1/2-associated ovarian cancer
LNG-IUS ↓ risk of endometrial cancer in general population
Aspirin
- ↓ risk of all types of cancer including Lynch syndrome carriers
- ↓ endometrial cancer risk in obese
- Smoking, alcohol & ↑ BMI → increase risk of colorectal cancer
 |
| Ref: TOG |
Gynecological surveillance in LS
- Not all want to undergo TAH+BSO
Fertility sparing surveillance — overall low quality evidence
- Aims to reassure or detect cancer early
- TVS Limited utility
- Hysteroscopy & endometrial biopsy Invasive; 30-40% complain of pain
 |
| Ref: TOG |
Fertility & LS
- No effect on fertility
- As it is autosomal dominant → 50% chance of passing defective gene to children affected
- LS is on list of conditions curated by HFEA
- Those affected with LS can access PGT before IVF which ↓ risk of transmission
- Uptake of PGT is variable as many couples prefer to conceive naturally
- Counsel them that risk of endometrial cancer rises sharply for women > 40yrs
Diagnosing LS in women with endometrial cancer
Clinical criteria
- Detailed family history MUST
- History-based prediction tools devised with different sensitivities and specificities —none is very reliable
- Best is to seek advice form clinical genetic service
- Women with LS develop endometrial cancer at an earlier age than sporadic tumors
- Endometriod endometrial & ovarian tumors→ most commonly associated with LS
Tumor-based testing
- Does not identify people with LS; it stratifies their risk for the condition
- Can be done without explicit consent
- Helps to identify who should undergo definitive but expensive germline testing
 |
| Ref: TOG |
Immunihistochemistry
- Loss of tumor expression of 1 or more MMR proteins (MMR deficiency)→ a feature of LS
- MMR protein immunohistochemistry for detecting LS associated endometrial cancer sensitivity 80-100% specificity 60-80%
- MLH1 methylation testing correctly identifies tumors caused by somatice methylation events
Microsatellite instability testing (MSI)
- Marker of hypermutation
- As LS tumors have multiple mutations so there is inevitable variation within tumor microsatellites
- If detected it is possible to diagnose through PCR
Genomic diagnosis
- Only means by which diagnosis of Lynch syndrome can be made
- Done using next-generation sequencing (NGS)
- Must have informed consent
- Not always straightforward
Targeted treatments in LS-associated gynae cancers
- MMR-deficient cancer are very immunogenic
- PD-1 checkpoint inhibitor Pembrolizumab: IgG4 isotope antibody which targets PD-1 receptor. (FDA approved USA)
You may also like
No comments:
Post a Comment