
This is a quick summary of the points taken from the TOG article which was published in July 2023. It is an important exam topic so must be covered thoroughly.
To download the original article: Click Here
To Access All TOGs: Click Here
To Join RK4 MRCOG Courses: Click Here

Introduction
- Tuberculosis (TB) is one of the leading infectious causes of overall mortality
- Highest disease burden in low-resource countries
- >2/3 cases in Africa and Southeast Asia
- Co-infection of TB & HIV in reproductive years is significant
- In UK — increasing due to immigration
- Can have adverse effects on mother & fetus
Epidemiology
- Global incidence - 1990-2020 — 9.9 million with 1.3 million deaths worldwide
- Major contributors to the resurging global TB epidemic — Poverty, HIV Coinfection, Drug resistance
- In 2020 UK had 4700 cases = 6.9 per 100 000
- Risk of new migrant women having active TB highest in first 5 years of migration
- Exact worldwide TB prevalence in pregnancy - Uncertain & depends on area
- Low-prevalence countries 0.06-0.25%
- High-prevalence countries
- 0.07-0.5% (in HIV negative)
- 0.7-11% (in HIV-positive)
Pathophysiology
- Causative organism — Mycobacterium tuberculosis (non-spore-forming, aerobic & non-motile bacteria)
- Primarily airborne infection
- Can also occur through ingestion of unpasteurised milk or direct implantation
- TB particles range from 1-5 microns in size, carried to terminal alveoli and multiply there
- Alveolar macrophages ingest & destroy most of the particles, but few survive and continue to multiply
- A granuloma is formed by macrophages around the bacilli
- Usually, the immune system clears the infection, but if it fails, it remains dormant without clinical manifestations or may cause symptoms.
- ~10% immunocompromised with latent TB will develop reactivation of TB
- ~10% healthy acquire infection during their life
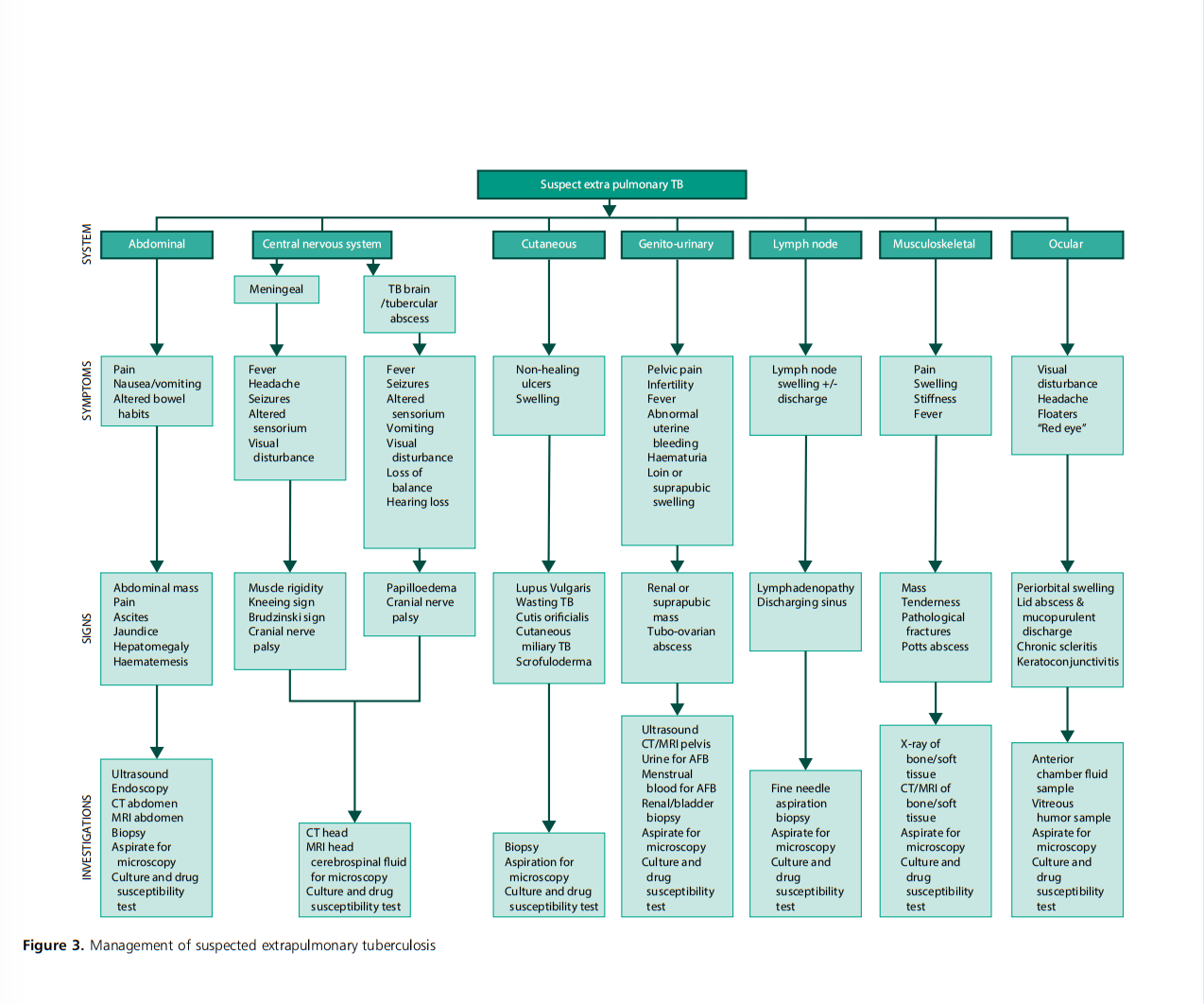
- Most common form of clinical TB — Pulmonary disease
- 20% active TB can present as extrapulmonary TB with cervical nodes being most common site (31%).
- Other sites are CNS, spinal cord, abdomen, pericardium (more common in immunocompromised & HIV-positive)
- Latent TB
- Primary TB (within 2 years)
- Secondary TB
Clinical Presentation
- Suspect TB if h/o exposure to patients with chronic cough or recent visits to endemic areas
- Symptoms except for Fever same as non-pregnant — weight loss, night sweats, chills, appetite loss, tiredness & weakness
- Latent disease will be asymptomatic & non-infectious but can have reactivation
- Four-symptom screening for TB suggested by WHO
- Fever
- Night sweats
- Cough
- Weight loss
Investigations
Screening tests
- TB skin test (TBT)
- Interferon gamma release assay (IGRA)
Confirmatory tests
- Microscopy
- Culture and sensitivity
Additional tests
- Imaging studies
Tuberculosis Skin Test (TST)
- Purified protein derivative (PPD) injected intradermally & delayed hypersensitivity reaction induration (5-15 m) measured at 48-72 hrs.
- No effect of pregnancy on results
- PPD safe for both mother & fetus
- Two types of TST : Tine (used rarely) and Mantoux (commonly used)
- False positive: with previous BCG vaccination, previous TB infection and infection with non-tuberculous mycobacterium
- False negative: due to technical issues, women with recent TB infection, immunocompromised, sarcoidosis, non-Hodgkin’s lymphoma, recent live vaccination with measles or chickenpox
Interferon-gamma release assay (IGRA)
- Detects interferon gamma
- Not influenced by BCG vaccination
- Not validated for use in pregnancy but performed routinely
- Can not differentiate latent from active infection
Microscopy
- Most commonly used to detect acid-fast bacilli (AFB) - Ziegle-Neelsen staining of sputum
- Sputum-positive detects 56 - 68% of pulmonary TB which means it may miss 1/3 of active cases
Culture and sensitivity
- Lowenstein-Jensen medium used traditionally
- Culture takes 4-8 wks Drug sensitivity a further 6-8 weeks
- Solid culture media now replaced by liquid culture media (BD-BACTEC & MGIT 960)
Imaging studies
Chest X-ray (CXR)
- Good screening tool
- Should be used in pregnancy when clinically indicated with proper shielding
- CXR can show healed lesions or a Ghon’s focus in treated cases
- 14% of culture-positive TB patients can have normal CXR
Ultrasound: Can be used safely
CT & MRI: Used if needed
Effects of Pregnancy on TB
- Pregnancy makes the diagnosis challenging
- Increased risk of reactivation in postpartum period (highly susceptible time)
- Prognosis depends on severity of disease, response to medicines, organs involvement and individual susceptibility
- HIV Coinfection more likely to progress the disease
- Timely diagnosis & prompt treatment improves outcomes
Effect of TB on Pregnancy
- Outcomes depend on disease stage, gestation at diagnosis, treatment, if extrapulmonary spread, coinfection with HIV and comorbidities like DM
- TB increase risks during pregnancy & postpartum
- Aneamia 41% (active TB) vs 23% (no active TB)
- Prematurity 32% SGA 22% Increased Oligohydramnios
HIV-TB Coinfection
- Challenging to diagnose and treat
- Higher risk of multidrug-resistant TB and disease relapse
- Risk of TB 21 times higher in women with HIV as compared to general pregnant women.
- HIV-TB con infection can lead to increased anaemia, eclampsia, placenta accreta, drug abuse and depression
Treatment of TB in pregnancy
- When treated earlier, associated risks almost eliminated
- Plan in collaboration with MDT
- Treatment initiated based on disease status

Ref: TOG
Active TB
- Start t/m as early as possible
- NICE: no difference in treatment, duration and dose in pregnant
- TB not involving CNS to be treated with
- Isoniazid, Rifampicin, Pyranzimide, Ethambutol — 2 months (initial phase)
- Isoniazid, Rifampicin — 4 months (continuation phase)
- Total duration of treatment — 6 months
- If CNS involved treatment for — 12 months (Same drugs 2 M + 10 M)
- Must give pyridoxine 10mg/day with isoniazid to avoid neurotoxicity to mother and baby
- Once treatment started, must have a follow-up to assess if converted to non-infectious
- NICE recommends fixed-dose daily dosing in all women
- If CNS involved, adjuvant corticosteroids with either dexamethasone or prednisolone recommended. Given over 4-8 wks with gradual dose tapering. Consider stress dose of steroids during labour.
- All first-line anti-TB drugs are FDA category C and are safe in pregnancy
- Avoid streptomycin which has 15% risk of neonatal irreversible deafness
Drug-resistant and multidrug-resistant TB
- Duration of initial t/m phase same 2 M but continuation phase varies 4-7 months
Latent TB
- Consider for prophylaxis if HIV positive, at high risk of acquiring recent TB or after investigations.
- Do not delay treatment until 2nd trimester
- For latent TB give isoniazid 6 months or combination of Isoniazid + Rifampacin for 3 months
- Must give supplemental pyridoxine with isoniazid
Perinatal TB
- Included TB acquired congenitally & postnatal
- Both have same treatment and prognosis
- Congenital TB — refers to acquiring TB by fetus in utero, either antenatal or intrapartum
- Neonatal TB — usually acquired in immediate postpartum period.
- The primary focus in neonates is on liver and periportal lymph nodes
- Military pattern is the most common finding on CXR in neonates
- Diagnostic criteria for perinatal TB
- demonstration of lesions in the new-born in the first week of life
- primary hepatic complex or caseating granuloma on percutaneous liver biopsy at birth
- placental or maternal genital tract TB
- excluding the likelihood of transmission by postnatal contacts
- Perinatal TB has high mortality rate for both treated 22% and non-treated 38%
- Treatment same as adults along with pyridoxine
- If active maternal TB and no clinical or lab evidence of prenatal TB, isoniazid preventive therapy at 10 mg/kg/day recommended for 6 months along with pyridoxine
- Breastfeeding to be commenced after MDT
- Anti-TB drugs considered safe if mother completed at least 2 weeks of treatment
- Breastfeeding usually not recommended for breast TB, multidrug or extended drug-resistant TB or co-infection with HIV
BCG vaccination
- Currently the only approved vaccine by WHO
- Single dose given to all neonates as soon as possible after birth
- In UK — BCG vaccine recommended for neonates whose parents or grandparents were born in a country where annual incidence of TB is ≥40/100 000 or newborn lives in an area of UK with annual incidence of ≥40/100 000
- Avoid BCG vaccine in pregnancy
- Contraindicated in infants exposed to immunosuppressant t/m in utero or in breastfeeding children with an active TB case suspected or confirmed in their household.
- HIV-positive mother — BCG to be given if child HIV negative at 12-14 wks & exclusively formula fed since birth
 |
| Ref: TOG |
 |
| Ref: TOG |

No comments:
Post a Comment