

TOG Article: Unscheduled bleeding with HRT
Volume 21, Issue 2 April 2019
- Menopause is diagnosed retrospectively AFTER 1 Year of amenorrhea in absence of hormonal contraception & any pathological disorder
- Average age: between 50-51 years (UK Median age 51 yrs)
Pathophysiology
- Biological ageing process has some changes in hormone levels
FSH: first to increase
Estradiaol: last hormone to decrease
Inhibin A & B: fall 2-3 years before menopause
- Cessation of ovarian function: FSH >50 mU/ml plus Estradiol < 20 pg/ml
- Perimenopause: Transitional period until menopause with irregular menstrual cycles
- PMB: any bleeding occurring after 1 year of menopause regardless of cause
- Perimenopause & postmenopause are associated with certain symptoms
Psychological:
mood swings, irritability, nervousness, dysphoria & decreased libido, depression, loss of cognitive function & insomnia
Vasomotor:
hot flushes (70-80% women experience it which gradually decreases, with only 25-30% after 5years), night sweats, headaches & palpitations.
Urogenital:
urogenital atrophy including a burning or itching discomfort in vagina, dysparunea & UTIs
Postmenopausal osteoporosis :
Postmenopausal osteoporosis :
HRT
- Prescribed after thorough risk assessment of VTE, CHD & breast CA
- Absolute contraindications:
- undiagnosed vaginal bleeding
- hepatic disorders
- acute vascular thrombosis
- HRT justified when QoL is adversely affected
- NICE: lowest effective dose to be used for shortest possible time, annually reviewed, continued as long as woman perceives benefit
- Options are
- estrogen only in hysterectomized or
- combined (estrogen+progesterone) with intact uterus
- Sequential Combined: continuous estrogen & cyclical progesterone for 12-14 days in a 28-day cycle. Regular monthly bleeds.
- Continuous Combined: daily estrogen & progesterone. Usually induces amenorrhea in 6 Months. Could be used in severe endometriosis.
- Routes: Oral, transdermal, subcutaneous, vaginal or intrauterine
Unscheduled bleeding with HRT
- Up to 80% experience unscheduled bleeding on combined HRT in first six months
- Evaluation must be after 6 months of HRT or after amenorrhea is established (which could be earlier than 6 months)
Prevalence (Important to remember)
- Combined Continuous (oral or transdermal) :
- 0-77% (in first few months)
- 3-10% in 9 months
- Transdermal: 10-20% after 1 year of use
- Sequential: 8-40%
- 25-50% women discontinue HRT due to unscheduled bleeding. More in White
Aetiology
- Presence of pathology: atrophic vaginitis, uterine polyps, fibroids, ovarian cysts or cancer, endometrial hyperplasia or cancer & de novo endometrial cancers
- Other causes: Poor/non-compliance; drug interactions e.g anti-epileptics; GI problems; obesity
- Many women have unscheduled bleeding without prevailing pathology
- Fast-tracked referral only if high-risk factors
Investigations
- Detailed history
- Menstrual diaries
- Most important reason to investigate is to rule out endometrial hyperplasia/ malignancy
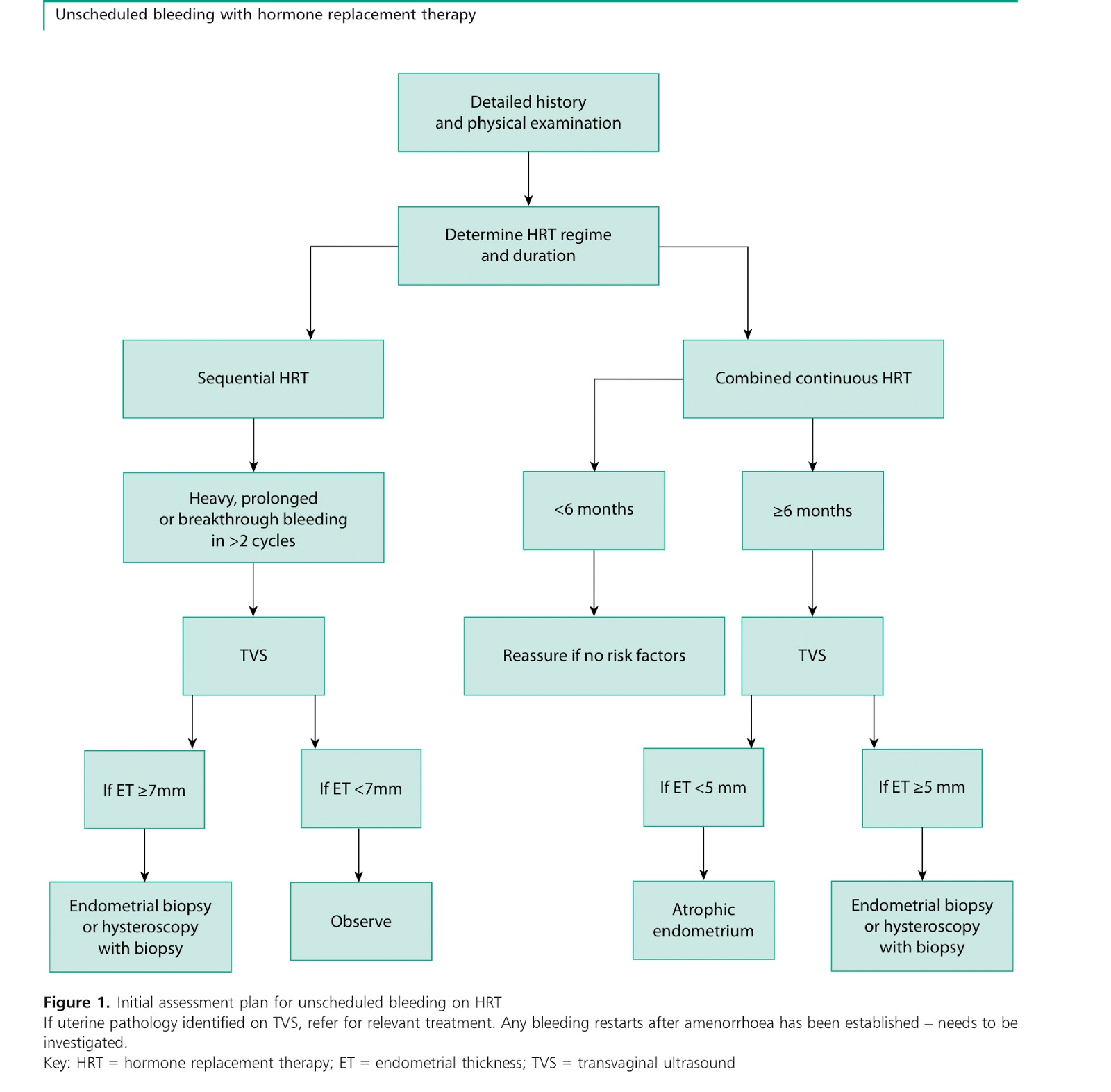
Initial Assessment plan:
 |
| Ref: TOG |
Hysteroscopy:
Gold standard for uterine cavity evaluation but not without risks
Criteria for Hysteroscopy
- Multiple bleeding episodes
- Focal lesions on transvaginal ultrasound
- Endometrial thickness (ET) >5 mm on continuous combined HRT and ET >7 mm on sequential combined HRT
- Incomplete visualization of endometrial echo or fragmentation of endometrial echo on ultrasound scan
- High-risk group with risk factors for endometrial disease or cancer (e.g. raised body mass index, family history of hereditary nonpolyposis colorectal cancer)
TVS
- Used as in initial tool in evaluation & safe + cost effective
- Sensitivity is not effected by hormonal use
- Allows to detect other pelvic pathologies as well e.g ovarian cysts
- <5mm endometrial thickness in PMB decreases the risk of endometrial cancer by 90% regardless of hormone use
- PMB + No HRT: pretest probability 10% & post test probability 1% (if test negative)
- PMB + Sequential HRT: endometrial thickness is greater than those who are not on sequential HRT
Referral Criteria for USG to check endometrial thickness
- Any bleeding after 6 months of continuous combined HRT even in low-risk women
- Bleeding after amenorrhoea has been established
- Any bleeding in first 6 months if any significant risk factors present
Pipelle endometrial sampling
- Histology gives definite diagnosis in PMB
- It can miss 20% of focal lesions if used alone
- Can be used as first -line investigation as detection rate is 99.6%
Further imaging
CT and MRI
Management
- Appropriate counselling
- Recommended HRT: Start with sequential therapy, then convert to continuous method 1 year past menopause
- 80% women will be menopausal at 54 years of age
Sequential HRT
- First rule out possible causes like poor compliance, drug interactions etc
- Check endometrial thickness with TVS within a week of last progesterone pill
- Heavy/prolonged withdrawal bleeding: Increase dose of progesterone / Change type of progesterone / Reduce dose of estrogen
- Bleeding in early progesterone phase: increase dose/change type of progesterone
- Spotting before withdrawal bleeding: Increase dose of estrogen
- Irregular bleeding: change regime / increase progesterone dose
- Painful bleeding: change type of progesterone
Continuous Combined HRT
- Investigate after 6 months or if bleeding starts after a period of amenorrhea
- Exclude endometrial pathology
- Lower estrogen dose
- Increase dose of progesterone /change type of progesterone
- If all fails, then to switch to sequential HRT
Other options
Intrauterine System
- Used for endometrial protection in women with estrogen only preparations
- Avoids systemic effects of progesterone, induces endometrial atrophy, causes regression of existing small polyps & reduces formation of new polyps
Topical vaginal estrogen
- Viable alternative in women with significant urogenital symptoms
- Not much risks associated
Surgery
- Endometrial ablation offered to women with poor response to other options
- After that endometrial protection must be offered
- Other options are hysteroscopic myomectomy/polyp resection
vaery much informative.Allah bless you. please could you continue give such summaies of other TOG in your spare time.
ReplyDeletejazak allah khairun
Thanks for appreciation. I am glad that you found it helpful. Hopefully I’ll continue with the other TOG summaries.
DeleteSo nice.Thank you
ReplyDeleteWelcome
DeleteVery well summarised. Thank you.
ReplyDeleteThanks for taking out time to go through this.
DeleteGood summary please solve cpd too with it
ReplyDeleteThanks a lot madam. God bless you! Please do the other TOGs as well.
ReplyDeleteDr Rubab, You are doing a wonderful job here. these summaries are quite good. I would like to make a little suggestion. Please improve the content covering answers for CPD questions as well. I noticed that some questions cannot be answered solely with the summary. And also we need to mention about sequential HRT when talk about the definition of PMB. Please make the addition.
ReplyDeleteOf course, your material is quite good and can easily cover the topic. Good luck & keep up the great service ! Really appreciate your work.
Appreciated
ReplyDeleteDr Rubab the CPD answers are also you provide ,and really much appricited help u are doing thanks again
ReplyDelete