
This is the summary of GTG -69 Hyperemesis Gravidarum released in 2016. This is one of a frequently tested guideline in the exam. Nausea and vomiting of pregnancy is one the most common indication for admission with typical stay of 3-4 days in the Hopsital. Hyperemesis Gravidarum is the severe form of NVP which can adversely affect the QoL and has a high recurrence in next pregnancy.
I hope this post is helpful. Suggestions to improve future posts are welcome.
Thanks
To download the full GTG 69 Click Here
All GTGs links Click Here

Epidemiology
NVP symptoms of nausea ± vomiting during early pregnancy where no other causes 80%
HG severe form of NVP 0.3-3.6%
Recurrence 15%-80%
- Reduced if change in paternity in second pregnancy 10.9%
Diagnosis of NVP & HG
NVP diagnosis ONLY when onset in 1st trimester + other causes excluded
- If after 10+6 wk→ consider other causes
- Typically starts 4-7th wk Peaks 9th wk Resolves by 20 wk in 90%
HG diagnosis Protracted NVP with triad of >5% pre-pregnancy weight loss, dehydration & electrolyte imbalance
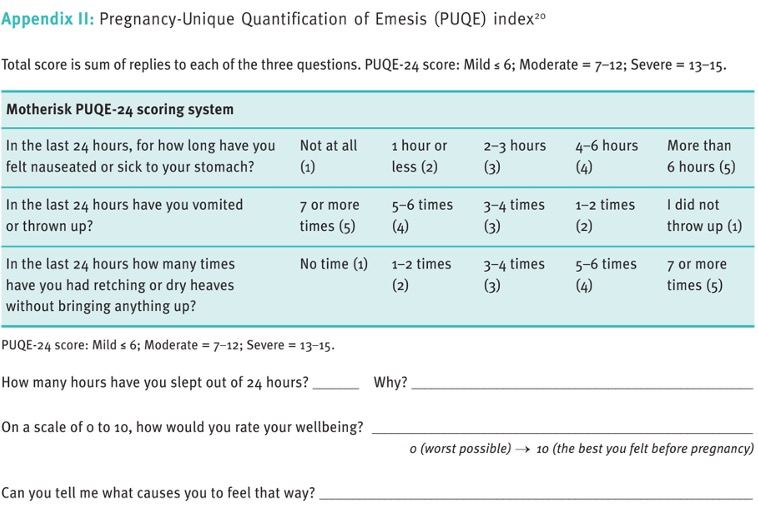
Severity NVP classify Objective & validated index of N & V PUQE Pregnancy Unique Quantification of Emesis
Initial clinical assessment & baseline investigations
- Features in history, examination & investigations to asses & diagnose NVP and HG for monitoring of the severity
History and Examination

Investigations

Urine dipstick quantify ketonuria as 1+ or more MSU
U&E hypo/hyperkalemia, hyponatremia, dehydration, renal disease
FBC infections, anemia, HCT
Blood glucose monitoring exclude DK if diabetic
USG confirm viability exclude multiple pregnancy & GTN
If refractory or h/o previous admission check TFT, LFT, Ca & Phosphate, Amylase, ABG
NVP & HG associated with
- Hyponatremia, hypokalaemia, low serum urea, including HCT & ketonuria→metabolic hypochloraemic alkalosis
- If severe→ metabolic acidaemia
TFT abnormal in up to 2/3 of HG 60%
- Biochemical thyrotoxicosis
- ↑free T4 ± suppressed TSH
- Clinically euthyroid
- Thyroid antibody rare
- Usually resolve as HG improve
- No need for thyroid drugs
LFT abnormal in up to 40% of HG
- Most likely ↑ transaminases
- Bilirubin slightly ↑ but no jaundice
- Amylase mild ↑
- All improve as HG improve
Differential diagnosis
- Peptic ulcer
- Cholecystitis
- Gastroenteritis
- Hepatitis
- Pancreatitis
- UTI or Pylonephritis
- Metabolic
- Neurological
- Drug-induced
Severe abdominal or epigastric pain unusual in NVP & HG→ warrant further investigations S amylase & USG
Gastroduodenoscopy Safe in pregnancy
Chronic infection with H.pylori Consider testing antibodies
Initial Management of NVP & HG

How woman should be managed? Main antiemetics, fluid replacement Thiamine
Mild NVP in community with antiemetics
Primary/community management fails or PUQE <13 Ambulatory day care management
Consider inpatient if any ONE of this
- Continued N&V → unable to keep down oral antiemetics
- Continued N&V + ketonuria ± wt loss >5% pre-pregnancy despite oral antiemetics
- Confirmed or suspected comorbidity (UTI, oral antibiotic intolerance)
Ambulatory day care provides parenteral fluid, vitamins & antiemetics
- Associated with high pt satisfaction
- Ambulatory s/c metoclopramide → 89.3% effective
Recurrent NVP & HG despite ambulatory daycare management inpatient especially if electrolyte imbalance or nutritional deficiencies
Therapeutic options
Antiemetics
- First line Antihistamines & Phenothiazines→ safe
- Use combination if do not respond to single
- With severe or persistent HG parental or rectal route is more effective than oral
- Drug-induced extrapyramidal symptoms & oculogyric crises with use of phenothiazine & metoclopramide promptly stop drug
- Clinicians should use antiemetics with which they are familiar
- Use different classes of drug if one not effective
Metoclopramide
- Safe & effective but extrapyramidal symptoms so use as 2nd line
- Only prescribe short-term
- 30mg/day or 0.5mg/kg in 24 hrs I/V → slow bolus inj over at least 3 min
- Maximum duration 5 days
Ondansetron
Safe & effective but limited data so use as 2nd line
Use should be limited to those not adequately management by other antiemetics & preferably after 1st trimester
Better at reducing N&V than doxylamine & pyridoxine
Equally effective but with less side effects than metoclopramide
More effective than metoclopramide in reducing severe vomiting
Safe drugs with no ↑ teratogenesis risk or other adverse effects
- Antihistamines promethazine, cyclizine, cinnarizine, doxylamine, dimenhydrinate
- Phenothiazines prochlorperazine, chlorpromazine, perphenazine
- Dopamine antagonist metoclopramide, domperidone
Pyridoxine
- Not recommended for NVP & HG
- Combination with doxylamine more effective than pyridoxine alone
Corticosteroids
- Reserved when standard therapies fail
- Rapid & dramatic improvements in women with refractory HG
- Daily I/V hydrocortisone 300mg → superior to I/V metoclopramide in reducing vomiting & recurrence
- Suggested dose 100mg I/V BD, once improved convert to 40-50 mg prednisolone daily, then taper off until lowest maintenance dose with controlled symptoms
Diazepam
- Not recommended
- Addition of diazepam reduces nausea but no difference in vomiting
Best Rehydration Regimen
- N.Saline + KCl in each bag + administration guided by daily electrolyte monitoring→ most appropriate I/V rehydration
- Dextrose do not give unless serum Na normal & thiamine given before (high doses 100mg/day parental to prevent Wernick's Encephalopathy)
Complementary therapies
Ginger
- May be used in mild to moderate NVP (multiple studies).
- No studies for ginger use in HG
- No ↑ risk of major malformations
- Potential maternal adverse effects anticoagulant effect, stomach irritation, potential interaction with ß blockers & benzodiazepines
Acustimulations--acupressure & acupuncture
- Reassure acustimulation safe in pregnancy
- Acupressure may improve NVP
- At pericardium 6 located about 2.5 fingers breadth up from wrist crease on inside of forearm b/w Palmaris Longus & Felxor Carpi Radialis tendon
Hypnosis
- Not recommended
Monitoring & adverse effects
Daily urea & electrolytes in pt on I/V fluids to prevent & treat hyponatremia & hypokalaemia
H2 antagonist or PPI in gastritis, reflux esophagitis.
Oesophageal gastroduodenoscopy safe, indicated if haematemesis or severe epigastric pain
Thiamine (oral or i/v) to ALL admitted with prolonged vomiting & especially before giving dextrose or parenteral nutrition
Wernick's Encephalopathy
- Vit B1 deficiency
- Classically presents with blurred vision, unsteadiness & confusion/memory problem/drowsiness
- On examination nystagmus, ophthalmoplegia, hyporeflexia or areflexia, gait ± finger-nose ataxia
- In HG episodic & slow onset
- Potentially fatal but reversible medical emergency
- Complete remission 29%
- Overall pregnancy loss 48% —including IUDs & TOP
Thromboprophylaxis LMWH in admitted with HG
- Continue for at least til 1st trimester
- OR for VTE with HG 2.5
- Adjusted OR of DVT 4.4
Previous or current NVP or HG Consider avoiding iron preparation —2/3 improvement
Further Management
Role of MDT
- Midwives, nurses, dietician, pharmacists, endocrinologist, nutritionists, gastroenterologists & mental health team including psychiatrists
- Mental health team involvement may improve QoL & ability to cope with pregnancy
Parenteral nutrition & feto-maternal risks
- Consider parenteral when all other medical therapies have failed after discussion at MDT
- No defined criteria
- Effectiveness not well established
- Often employed as last resort
- Enteral feeding options nasogastric, naso-duodenal or naso-jejunal tubes or percutaneous endoscopic gastrostomy or jejunostomy feeding
- Peripherally inserted central catheter PICC line parenteral feeding better tolerated than enteral feeding but high risk of infection & vascular perforation
- Intra-gastric feeding ok for short term but ↑ risk of N&V
- Naso-jejunal tube put endoscopically to jejunum & continuous infusion for feeding. Great improvements within 48hr
- Percutaneous endoscopic gastrojejunostomy feeding under GA in 2nd trimester effective, safe & well-tolerated.
- TPN complex high-risk intervention
- Useful in refractory cases to ensure adequate calorie intake
- Only a last resort because expensive, inconvenient, associated with serious complications like thrombosis, infection & metabolic disturbances
- Associated with↓ perinatal mortality
- Strict protocol with careful monitoring essential
When should TOP be considered?
- All therapeutic measure should have been tried before offering TOP of a wanted pregnancy
- Consider all t/m options before decision
- Psychiatrist opinion should be sought
- Decision at MDT with documentation of therapy failure
- Counselling before & after the decision
Prominent reasons
- 66% unable to maintain self & family care
- 51% fear of baby or self dying
- 22% think baby would be abnormal
Discharge & follow-up
- Individualised management plans
- If NVP & HG continued in late 2nd or 3rd trimester offer serial growth scans
- Patient support groups
- Follow-up appointment
- Psychological & social support
Complications in Pregnancy
- HG & low pregnancy wt gain ↑ risk of preterm delivery & LBW
- Excessive vomiting lasting beyond 5M associated with underweight children
- Repeated admission 18% incidence for SGA & LBW
Effect of NVP & HG in postnatal time
- Advice about risk of recurrence 15 – 81%
- Early lifestyle/diet modification & antiemetics which were useful in index pregnancy advisable to reduce NVP & HG in current pregnancy
Effects of NVP & HG on QoL
Women with HG
- 3-6 times more likely than NVP to have low QoL
- Persistent nausea most adversely affect QoL
- significantly higher somatisation, depression, anxiety & overall psychological distress even when HG resolved to mild NVP
- Symptoms of major depression associated with moderate & severe NVP but prior h/o depression not a determinant
- More depression & anxiety if they feel that healthcare professional is unsympathetic
Having support from at least 3 other persons protective for NVP
You may also like:
GTG 38 Management of Gestational Trophoblast Diseases 2020
GTG 26 Assisted Vaginal Birth 2020
LIVE Session Early Pregnancy Care 2021
Module 16 Early Pregnancy Care
Hi Dr. Rubab
ReplyDeleteThis is extremely helpful. I wonder if there are such summaries of other guidelines and tog/sip also. Moreover i would like to know if you run any course for MRCOG 2 preparation?
Thanks.
Regards
Hi Mary!
DeleteI am glad you found it helpful. Yes other guidelines have also been summarised and available in blog archive. Currently the course for MRCOG part 2 July exam is going on.
Please visit this link for further details:
http://www.rubabk4courses.com/courses/
Regards
Hello Dr. Rubber, it extremely helpful thank you ma'am 😊
ReplyDelete