
The points in this post have been extracted from a TOG article published in April 2021. Surgical site infection poses a challenge for surgery and has huge impact on patient care/safety and healthcare system. It is an important cause of patient morbidity and if severe can even lead to death.
Different guidelines have been produced to address this issue. This article provides a very good resource of comprehensive information about SSI.
It is recommended to read the original article to grasp the topic completely.
I hope you find this post helpful.
Suggestions to improve future posts are welcome.
Thanks
 |
| https://www.rubabk4courses.com/courses/ |
Introduction
- SSI remains a peri-surgical problem
- May lead to severe morbidity & mortality, prolonged hospitalisation & enormous economic costs
Measure to reduce SSI
- Improved ventilation in OTs
- Equipment sterilisation
- Barrier use during surgery
Factors which increase SSI
- Antibiotic resistant pathogens, chronic disorders like DM, alcoholism, obesity & immunosuppression
- In obstetrics SSI associated with prolonged labour, emergency CS & multiple vaginal examinations
- Common pathogens include gram +ve & -ve organisms such as Staphylococcus aureus & E. Coli
Definition
- Infection of superficial or deep skin incision, or of an organ or space, occurring up to 30 days after surgery if no implant was left behind, or within 1 year if an implant was left in place
Specific Criteria for diagnosis
Superficial wound infection at least one of the following
- Purulent effluent or exudate with organisms identified
- One of following: pain, redness, localized swelling, tenderness or heat
- Diagnosis by surgeon or attending physician
Deep wound infection at least one of the following
- Purulent exudate from deep wound incision
- Spontaneous dehiscence of deep incisional wound or if deliberately opened with temp >30˚C, localized pain or tenderness
- Abscess or infection involving deep wound incisions
- Diagnosis by surgeon or attending physician
Organ or space infection at least one of the following
- Purulent exudate from a drain
- Organism isolated
- Evidence of abscess or infection
- Diagnosis by surgeon or attending physician
Wound Classification
 |
| Ref: TOG |
Epidemiology
- Incidence 2-6% of surgeries in high-income countries
- UK in 2006 survey
- Incidence of health care-acquired infection 8% out of which 14% were SSI
- 5% patients having surgery had SSI
- Incidence varies according to the type of surgery
- Highest after bowel surgery 8%
- Lowest after knee replacement 0.5%
- After TAH 1.6%
- After CS 3-15%
Risk factors
 |
| Ref: TOG |
Microbiology
 |
| Ref: TOG |
- Various organisms responsible for SSI
- Some are endogenous normally present on the skin, in GI & genital tract
Most common causative pathogens
- Enterobacterales (AKA enterobacteriaceae), Staphylococcus aureus and coliforms such a E Coli & Proteus mirabilis
- NHS-wide audit of SSI percentage of organisms responsible
- Enterobacterale 30% S.aureus 23% Coliforms 19% P. miribilis 13%
- The proportion of SSI associated with S.aureus & MRSA/MSSA has increased over time.
In obs & gynae the microorganisms most frequently responsible for SSI are polymicrobial aerobes & anaerobes (from skin/ genital tract flora)
- Gynaecological SSI most likely secondary to Gram-negative bacilli, enterococcus, group B haemolytic streptococci and anaerobes
- Genital infections like bacterial vaginosis, Neisseria gonorrhoea, Chlamydia trachomatis or mycoplasma can lead to ascending infections after procedures through cervix/vagina
Organisms responsible after
- TAH → S. Aureus, E.coli and anaerobes
- CS → S. Aureus 40% Others E.coli 13%, Streptococcus sp. 7%, Enterococcus sp. and pseudomonas sp.
Prevention
Different guidelines

Patient factors
Identifying & managing modifiable risk factors reduces SSI incidence
- Adequate glycemic controls, avoidance of immunosuppressives, good nutrition and optimal Hb can help in wound healing and decrease SSI
- Reduce the hopsital stay duration
Preoperative factors
Nasal decolonization
- Good practice to screen for MRSA status
- Decontaminate (with mupirocin) before undergoing Obs & Gyn surgery
Patient & staff gowns
- Recommended for patients to wear comfortable & appropriate dressing for surgery with adequate exposure to surgical site
- Staff not actively involved in surgery to wear non-sterile theatre gowns
Preoperative bathing
- Recommended good practice to have preoperative bathing/showering as it reduces skin colonization by flora, especially at surgical site
- Time: the day before or on the day of surgery
- Use plain or an antimicrobial soap
- Use chlorhexidine if S.aureus likely cause of SSI in procedure and if MRSA carrier
- NICE same above recommendations
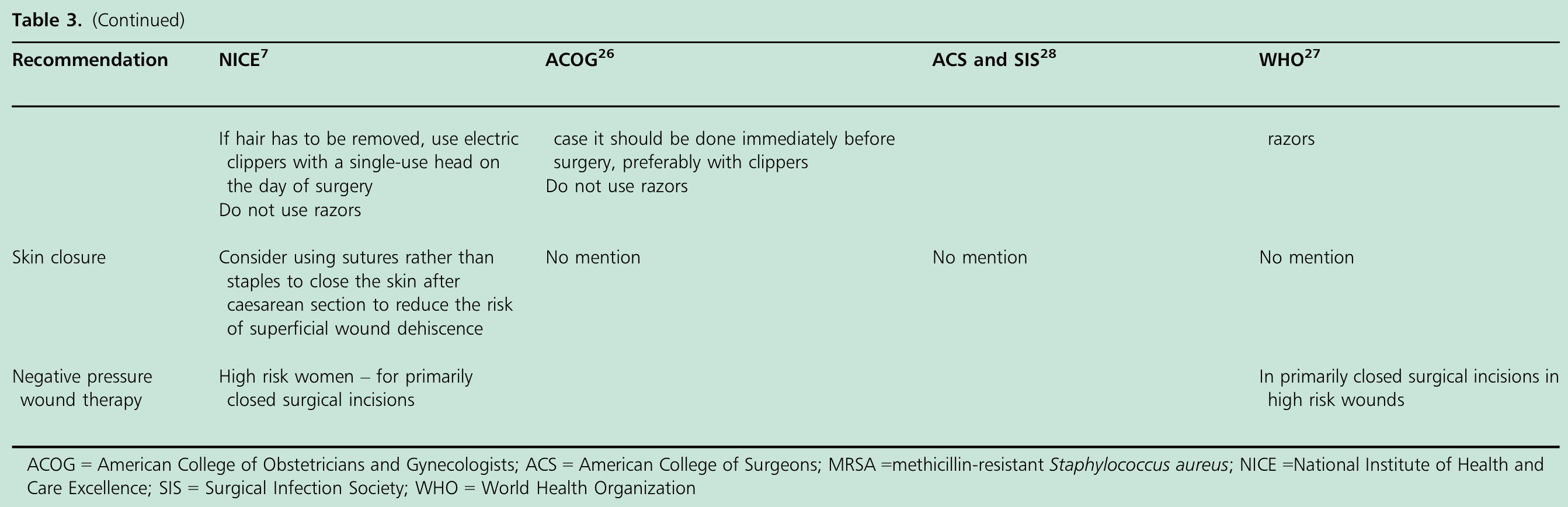
Hair removal
- Now becoming less common practice
- Can use razor, clipping or depilatory creams
- No advantage of any one technique over another
- WHO recommends to use Clippers for hair removal. Shaving discouraged strongly
- NICE discourages routine preoperative hair removal; if needed should be done by electric clippers
- Time: no difference in day before or on the day of surgery
Antimicrobial prophylaxis for CS
- SSI rate 68/1000 with antibiotics 97/1000 without antibiotics
- Prophylactic antibiotics reduces the incidence of SSI, endometritis and serious maternal infectious complications by 60-70%
- First generation cephalosporins reduce postoperative wound infection by 62% & endometritis by 58%
- IV antibiotics within 60 min of CS decreases composite maternal infectious morbidity by 53%, endometritis by 56% and wound infection by 41%
- Avoid augmentin before cord clamping
Antimicrobial prophylaxis for hysterectomy
- Overall prophylactic antibiotics reduce the risk of postoperative infection from 16% to 1-6%
- To be given within 60 minutes of skin incision
- NICE single dose of IV prophylactic antibiotic at induction of anaesthesia
- Usually recommended for surgeries with clean, clean contaminated and contaminated wounds
- If wound infected use prolonged antibiotics
- Prolonged surgery associated with increased rates of SSI
- SSI rate 6% for surgery <1 hr and 28% for surgery >2hrs
- Re-dosing is recommended if
- Surgery >3hrs and
- Blood loss >1500 ml
- Consider higher (or double) the standard dose for morbidly obese
- Prophylactic antibiotics not recommended in clean, non-prosthetic, uncomplicated surgeries like diagnostic laparoscopy, ovarian cystectomy or laparoscopic sterilization
 |
| Ref: TOG |
Intraoperative factors
Hand washing
- Using chlorhexidine or providine before surgery reduce the resident skin flora & SSI
- Recommended for surgical teams hand washing with antiseptic solution & single-use nail bruish before first operation
- Later, can use either alcoholic hand-rub. If soiled use antiseptic solution
- Hand-scrubbing for a minimum of 3 minutes reduces colony-forming units of microorganisms
Gloves
- Use of double gloves recommended for surgeon as it reduces SSI & needle stick injuries
Gowns and drapes
- Use as good practice as it reduces contamination of surgical field with possible source of infection
- No difference in SSI with either disposable or reusable drapes
- Iodophors-impregnated incise drapes better
Skin preparation
- Skin antiseptics reduce number of microflorae
- Chlorhexidine - Bacteriostatic
- Alcohol-based preparations —Bactericidal & evaporate quickly
- Undergoing CS: Alcohol-based Chlorhexidine is superior to providine-iodine
- For TAH: Chlorhexidine-alcohol
- Overall reduction in SSI 50%
- Significantly more protective than providine-iodine against both superficial / deep incisional infection but not against organ/space infections
- NICE recommends skin preparation with alcohol-based chlorhexidine before skin incision and to ensure that solution dries & evaporates before diathermy use
- If chlorhexidine contraindiacted→ use alcohol-based providine-iodine as second-line
- Waiting for 3 minutes for skin preparation to dry reduces the load of colony-forming units of bacteria
- Apply chlorhexidine-alcohol solution for 2 minutes for moist sites and 30 seconds for dry sites and allow to dry for 3 minutes
- Use aqueous solution of chlorhexidine in surgery near to mucous membranes
Vaginal preparation
- Vaginal preparation immediately before CS significantly reduces incidence of post-CS endometritis from 8% to 4%
- Risk reduction greatest for women already in labour & with ruptured membranes
- Not yet recommended by NICE
Skin incision
- Joel Cohen incision associated with less postoperative pain, fever, analgesic requirements & blood loss as well as short operating time & hospital stay
- No difference in SSI incidence as far as type of incision is concerned
Negative pressure wound therapy (NPWT)
- Vacuum dressing applied to promote wound healing
- Stimulates formation of granulation tissue, increases blood flow, reduces edema, improves wound contraction and protects against external contamination
- Reduces bacterial contamination & increases vascular perfusion / lymphatic clearance around surgical sites
- Lower SSI with NPWT 12% vs 27%
- Recommended by NICE specially to be used in patients at increased risk of SSI ; smokers & in advanced age
Intra-caesarean section procedures and SSI
Closure of uterine incision and peritoneum
- No effect on rate or SSI
- One or two layer closure of uterus
- Closure or non closure of peritoneum
- Adequate haemostasis & minimal use of drains reduces SSI
Subcutaneous tissue closure
- Reduces rate of haematoma or seroma formation
- Only beneficial if SC fat is >2cm deep
Wound closure and dressing
- Subcuticular closure→ less wound infection, better wound apposition & decreased rates of wound separation
- Antimicrobial coated sutures such as triclosan may reduce risk of SSI
- Wound dressings absorb wound exudates, reduce postoperative pain, provide moist environment & reduces exposure of wound to pathogens
- NICE advices against use of staples after CS and recommends use of appropriate interactive wound dressing
Special circumstances
Gynaecological oncology
- Principles are same
- Use of surgical site infection bundles — elements are following
- Antimicrobial prophylaxis Skin preparation Avoiding hypothermia & surgical drains Reducing intraoperative hypoglycemia
- Anaerobic coverage recommended if bowel entered during surgery
- Dosing to be based on weight and re-dosing considered based on duration of surgery and blood loss
- Maintenance of normo-thermia during surgery
- Drains & tubes not recommended in routine
- NG tube increases the risks
Immunosuppressive patients
- Must be screened for opportunistic & asymptomatic infections
Co-existing lower genital tract infections
- Minimize avoidable factors
- Treat coexisting infection before surgery. May use full treatment course along with prophylactic antibiotics
- If found incidental BV must be treated for 5-7 days prior to surgery
Postoperative factors
- Use aseptic non-touch technique for changing or removing dressings
- Wound cleansing with sterile saline for up to 48 hours
- Patient can shower safely after 48 hours of surgery
- If wound separated or opened to drain pus, tap water should be used to clean it after 48 hours
- Prolonging use of prophylactic antibiotics does not reduce SSI and not recommended
- Immobilization & prolonged hospital stay are risk factors for SSI. Follow enhanced recovery pathways
Management of SSI
- SSI typically develops within 4-7 days postoperatively specially after CS
- Symptoms of SSI fever, purulent discharged and other signs of inflammation
- Superficial wound infection→ erythema and tenderness with induration at site of infection
- Endometritis→ abdominal pain, heavy lochia, abnormal vaginal discharge ± purulent discharge
- Crucial to keep a high index of suspicion
- Asked on history, examination and review of vital signs
- Must evaluate for infection if any fever >38˚ C on at least two occasions, at least 4 hours apart more than 24 hours after surgery
- Not every SSI needs antibiotics treatment
- Minor or superficial infection may only need suture removal, abscess drainage & topical antiseptics
- Mainstay of treatment → use of antibiotics (broad-spectrum) after microbiological swabs
- Do not delay antibiotic treatment for tests
- Imaging may be needed to exclude inter-abdominal collection (TVS or CT)
- Consider imaging if persisting fever (not responding to 48 hrs of treatment) occurring more than 24 hours after surgery + with no identifiable source
- First line antibiotics → typically combination of penicillin (co-amoxiclave or cephalosporins + metronidazole). Covers S. Aureus and anaerobes which are most common cause of SSI
- If sever allergy to penicillin—can use Clindamycin or Vancomycin
- After hysterectomy, common SSI are
- Vaginal cuff and pelvic cellulitis and pelvic abscess
- May have fever, purulent discharge, erythema, hyperaemia and edema at the vault
- Might be self-limiting without need for antibiotics
- Superficial incisional SSI (wound infection)
- Most commonly caused by S.aureus
- Presents as cellulitis
- Treatment Flucloxacillin (clindamycin or vancomycin if allergy)
- Deep-seated SSI (pelvic cellulitis or pelvic abscess)
- May need surgical exploration & drainage as well as peritoneal saline wash with insertion of a drain
- Wound management should be in collaboration with tissue viability team
Necrotising fasciitis
- Uncommon SSI 1.8 in 1000 after CS
- Commonly caused by polymicrobial organisms; aerobic, a aerobics or mixed
- Three types
- Type I or Polymicrobial
- Type II or groups A streptococcal
- Type III gas gangrene
- Type II is the most common in Obs & Gynae, in patients with immunosuppression, DM, vascular insufficiency, chronic alcoholics, having transplant or using steroids
- High index of suspicion is critical to diagnosis
- Typical presentation: pain out of proportion with clinical signs
- Imaging may help
- Mainstay of treatment → antibiotics (early as it is a rapidly progressing condition)
Conclusion
- Key to reduction of SSI is prevention including modification of patient-related factors, preoperative optimism, peri- and intra-operative measure, aggressive postoperative vigilance and treatment of infec
You may also like
No comments:
Post a Comment