This blog post is based on the points taken from TOG article Non-epithelial Ovarian Cancers published in July 2021. This article provides a detailed review to understand the classification, diagnosis and management of all NEOCs with focus on MOGCTs and SCSTs.
I hope you find this post helpful.
To access the original article : Click Here
To access all TOG topics : Click Here
Introduction
Ovarian Cancer in UK
• 6th commonest cancer in women
• Causes 4000 deaths per annum
Non-epithelial ovarian cancers NEOCs
• uncommon form of ovarian tumor
• 10% of all ovarian malignancies
• NEOCs can present at ANY age
• Classified into
• Malignant Ovarian Germ Cell Tumors - MOGCTs
• Sex Cord-Stromal Tumors - SCSTs
• Ovarian Sarcoma
• Small cell carcinoma of the ovary
Pathophysiology
• Ovaries divided into cortex and medulla
• Cortex made of ovarian follicles, interstitial gland cells & stroma
• Surrounded by dense capsule and surface covered with surface epithelium (coelomic)
• Epithelial ovarian tumors occur due to neomataplasia of surface epithelial cells
• SCSTs arise from different cell types from primitive sex cords and stromal cells
• Stromal cells include→ Theca cells, Fibroblasts & Leydig cells
• Primitive sex cords include→ Granulosa & Sertoli cells
• Germ cells arise from endodermal layer of the yolk sac
• Most non-epithelial ovarian tumors arise from these above specific cells (germ cells, granulosa cells, theca cells, stromal fibroblasts and steroid cells)
Clinical Presentation
• The commonest presenting symptoms — persistent abdominal distention, pelvic or abdominal pain, urinary urgency or frequency & menstrual irregularities
• In female of ANY age presenting with complex ovarian mass — must consider NEOC as differential diagnosis
Classification of Non-epithelial Ovarian Cancer
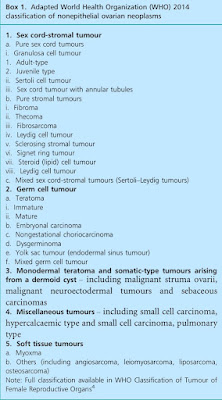 |
| Ref: TOG |
MOGCTs
• Usually occur in premenopausal women
• 80% of preadolescent ovarian malignancies
• Incidence 3.7 per 100 000 women per year
SCSTs can present at ANY age
• Adult-type granulosa cell tumors mainly in peri-menopausal & postmenopausal
• Sertoli-Leydig cell tumor occur in young
• Incidence 2.1 per 100 000 women per year
Malignant Germ Cell Tumors